
TMS for Anxiety: Does It Actually Work?
- Sophroneo Psychiatry

- Jun 8
- 5 min read

TMS is best known for depression, so many people with anxiety assume it is not relevant to them. That assumption can close a door too early. Anxiety is not just "overthinking." It involves brain circuits that detect threat, regulate attention, control physical arousal, and help the body come back down after stress.
Transcranial magnetic stimulation, or TMS, may help some anxiety symptoms by strengthening the prefrontal control systems that quiet the brain's alarm response. The evidence is still more established for depression than for anxiety alone, and generalized anxiety treatment with TMS may be off-label depending on the diagnosis and protocol. Still, for people whose anxiety has not improved enough with medication, therapy, or lifestyle changes, the question is worth asking carefully.
This article is educational and is not a substitute for diagnosis, treatment advice, or a personalized TMS plan. If anxiety comes with thoughts of self-harm, inability to sleep for days, panic that feels medically unsafe, or thoughts of suicide, call or text 988 in the U.S. or go to the nearest emergency department.
If you are exploring care, start with Sophroneo Behavioral Health & TMS and the clinic's dedicated page for anxiety treatment. Those pages can help you separate general anxiety education from a real psychiatric evaluation.
What TMS is doing in an anxious brain
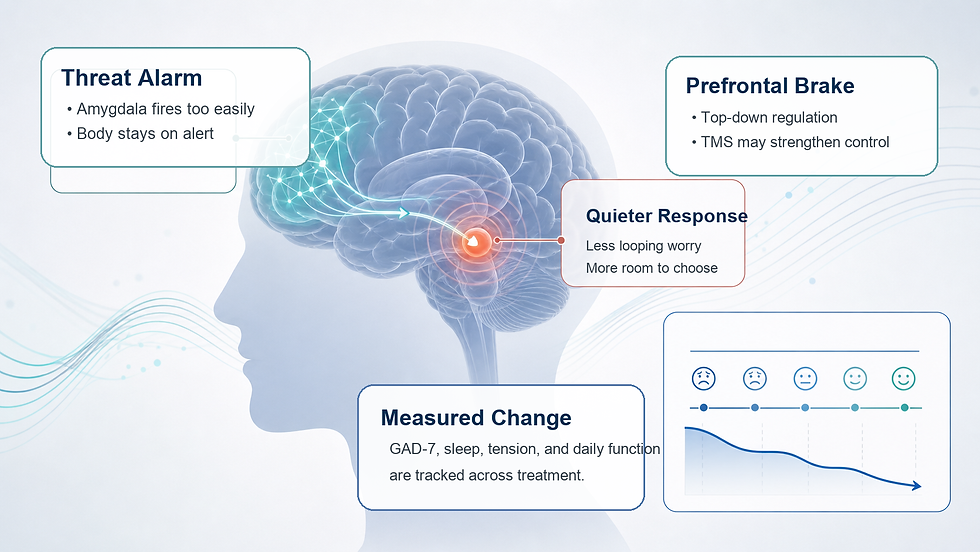
Anxiety often involves an overactive threat system and an underpowered regulatory system. The amygdala behaves like an alarm. The prefrontal cortex helps decide whether the alarm fits the situation. When the prefrontal cortex is not regulating effectively, the alarm keeps ringing even when there is no immediate danger.
TMS uses magnetic pulses to stimulate targeted areas of the cortex. For anxiety, many protocols focus on the dorsolateral prefrontal cortex because it helps regulate worry, attention, physical tension, and emotional reactivity. Some approaches use high-frequency stimulation on the left side, low-frequency stimulation on the right side, or a bilateral plan depending on the person and the condition being treated.
This is one reason anxiety and depression often get discussed together in TMS care. The same prefrontal circuits can be involved in low mood, rumination, insomnia, and chronic worry. Sophroneo's guides to how TMS works and NeuroStar TMS explain the treatment mechanics in more detail.
What the evidence suggests about TMS for anxiety
The research on TMS for anxiety is promising but uneven. Some studies and clinical programs report meaningful reductions in anxiety symptoms, especially when anxiety is part of a broader picture that also includes depression, PTSD, OCD, or sleep disruption. Other cases require careful protocol selection and realistic expectations.
For a person with generalized anxiety, useful tracking usually includes more than a vague "I feel calmer." Clinicians may use tools like the GAD-7, sleep logs, physical tension ratings, panic frequency, or functional markers such as work performance and avoidance. If symptoms improve, the change is often gradual rather than instant.
If anxiety is tangled with mood symptoms, review Sophroneo's page for depression treatment and its guide to depression symptoms, antidepressants, and TMS. If sleep is a major driver, the insomnia service page is also relevant.
Who might be a better candidate
TMS may be worth discussing when anxiety has persisted despite appropriate first-line care. That might include therapy, medication trials, sleep work, stress reduction, or treatment for co-occurring depression. The fit is stronger when symptoms suggest a brain-regulation pattern rather than a short-lived stress response.
People with physical tension, racing thoughts, sleep disruption, avoidance, and chronic hypervigilance may have a profile worth evaluating. Anxiety can also overlap with PTSD, OCD, ADHD, and depression, so a good consultation should not treat the diagnosis as one isolated label.
The broader Sophroneo services menu can help you identify which symptoms belong in the same conversation. For related reading, see the clinic's articles on natural anxiety remedies, breathing exercises and grounding for anxiety, and nighttime anxiety with racing thoughts.
How Sophroneo frames TMS for anxiety
At Sophroneo, the question is not whether TMS is a trendy anxiety treatment. The question is whether your anxiety pattern, treatment history, safety profile, and goals make TMS a reasonable part of care.
A careful evaluation should ask what has already been tried, what helped, what caused side effects, whether depression is present, whether trauma symptoms are active, whether sleep is destabilizing the nervous system, and whether medication management still has room to improve. It should also explain what TMS can and cannot promise.
If you are comparing treatment routes, the pages on whether TMS is right for you and what TMS feels like can help you ask more specific questions during a consultation.
A short anxiety primer before your visit
The video below is not a TMS protocol guide, but it gives a clear overview of generalized anxiety warning signs that can help you describe symptoms more precisely before meeting with a clinician.
What to expect if anxiety is your main symptom
Expect the consultation to be specific. A provider should ask about symptom severity, triggers, medication history, therapy history, sleep, panic symptoms, trauma symptoms, compulsions, medical conditions, and seizure-risk factors. If TMS is recommended, the protocol and tracking plan should be explained in plain language.
It is also fair to ask what outcomes the clinic tracks, how often scores are reviewed, and what happens if symptoms improve only partially. TMS is not a replacement for therapy or lifestyle support. For many people, it works best as part of a broader plan that makes therapy, sleep routines, medication management, and daily functioning easier to sustain.
Frequently asked questions
Is TMS FDA-approved specifically for anxiety?
TMS has FDA-cleared uses for conditions such as major depressive disorder and OCD. Use for generalized anxiety may be off-label, depending on diagnosis and protocol. Off-label treatment is common in psychiatry, but it should be explained clearly before you begin.
Can TMS make anxiety worse?
Some people notice temporary irritability or increased anxiety early in treatment as the brain adjusts, but serious adverse events are uncommon. A provider should review seizure history, medications, metal implants, and other safety factors before recommending TMS.
How long does TMS take to help anxiety?
Many people who respond notice changes gradually over several weeks rather than immediately. Sleep, physical tension, and rumination may shift before the person feels fully calmer.
Do I stop anxiety medication during TMS?
Usually, no. Many patients receive TMS while continuing prescribed medication. Any medication change should be planned with the prescribing clinician.
What should I ask a TMS provider about anxiety?
Ask what protocol they use for anxiety presentations, how they track outcomes, what diagnoses they commonly treat with TMS, what side effects to expect, and what the next step is if your anxiety improves only partially.



Comments